Blog

Is It a “Cute” Lisp, or Is It Time to See a Fort Myers Speech Therapist? The Sound-by-Age Timeline
It’s often endearing when a three-year-old announces she wants “pasketti” for dinner, or a kindergartner tells a long story in which every “r” comes out sounding like a “w.” It can also be the kind of occurrence that quietly plants a seed of curiosity in a parent’s mind: is this normal? Should something be happening by now? As Fort Myers speech therapists, we assure parents that most speech sound errors in young children are entirely typical. Children do not arrive in the world producing perfect sounds, and the journey toward clear speech follows a predictable developmental sequence.
However, it is also true that some errors do persist beyond the age when they should naturally resolve. When that happens, the earlier a child receives support, the better the outcomes tend to be.
This guide walks through the research-backed timeline of speech sound development, identifies the sounds that parents most commonly ask about (including the lisp, the “w” for “r” swap, and the elusive “th”), and explains what a Fort Myers speech therapist at FOCUS looks for when evaluating a child’s articulation.
Why some speech sound errors are developmentally normal
Your child’s Fort Myers speech therapist may explain that speech sounds are produced through an intricate coordination of the lips, tongue, teeth, palate, jaw, and airflow. Producing them accurately requires both motor learning and auditory discrimination, the ability to hear the difference between how a sound should sound and how it currently comes out. Children develop these skills gradually, and different sounds require different levels of motor precision.
The earliest sounds to emerge are those that require the least precise mouth movement: sounds like /m/, /b/, /p/, and /w/ involve the lips coming together in simple, visible movements. Later-developing sounds like /r/, /l/, /s/, and /th/ require the tongue to position itself in very specific ways that children cannot always coordinate on demand, even when they hear the sound correctly. This is why a child can hear the difference between “run” and “wun” perfectly well and still produce the second version consistently for years.
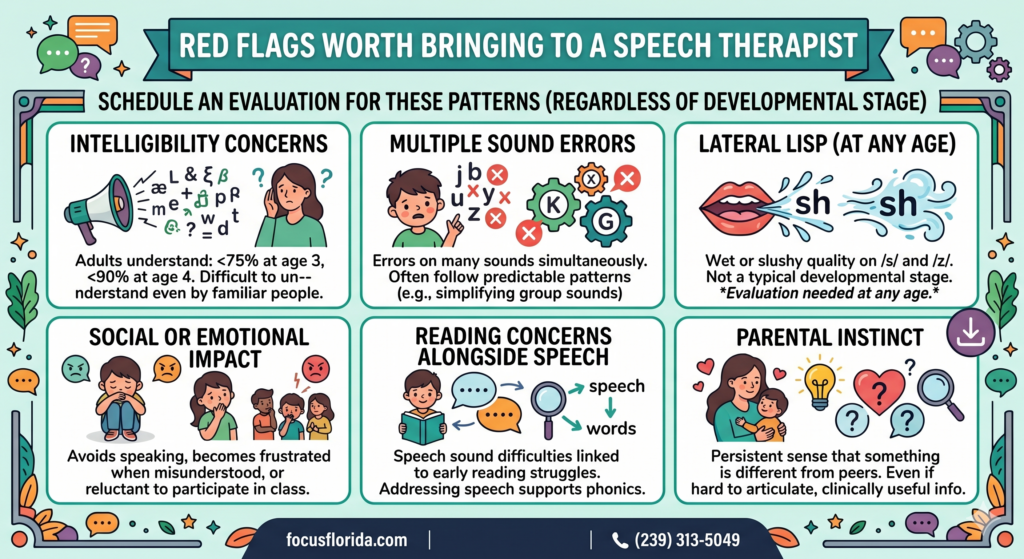
A speech sound error is considered developmentally appropriate when it is consistent with what most children that age are doing. It becomes a clinical concern when it persists significantly beyond the typical age of acquisition, or when it is affecting a child’s intelligibility, confidence, or willingness to communicate.
The speech sound acquisition timeline
The chart below reflects widely used norms from speech-language pathology research, including data from the landmark studies by Shriberg and McSweeny, as well as more recent normative research. Ages reflect when approximately 90% of children have mastered each sound, meaning consistent and accurate production across most contexts. Some individual variation is normal.
The speech sounds parents ask about most
The lisp: frontal vs. lateral
The word “lisp” gets used loosely to describe any distortion of the /s/ or /z/ sound, but there are actually two distinct patterns, and they have very different clinical implications.
A frontal lisp occurs when the tongue protrudes between the front teeth, producing a “th”-like sound instead of /s/. This pattern is developmentally normal in children under four to four and a half years old, because many young children are still learning to keep the tongue behind the teeth when speaking. A frontal lisp that persists past age five is worth evaluating, but it is also among the most responsive to speech therapy when addressed.
A lateral lisp is different in character. Here, air escapes over the sides of the tongue rather than straight through the center, giving /s/ and /z/ a wet or slushy quality. Unlike a frontal lisp, a lateral lisp is not a typical developmental stage at any age. When a lateral lisp is present, evaluation is generally recommended regardless of the child’s age.
The /r/ sound: why it takes so long and why it matters
The /r/ sound is one of the most acoustically complex sounds in American English and one of the most frequently misarticulated. It requires a very specific tongue body position that is largely invisible from the outside, which makes it harder for children to self-correct through imitation alone. Many children substitute /w/ for /r/ well into first and second grade, which is within normal developmental range.
By age seven, however, a persistent /r/ error begins to affect intelligibility and can become a real source of social difficulty. Children notice, other children notice, and classroom participation can be affected. The good news is that /r/ responds very well to targeted speech therapy, particularly when treatment begins between ages six and eight, before compensatory patterns become deeply established.
The /s/ and /z/ sounds: school age is the turning point
Because /s/ appears in so many English words, errors on this sound have an outsized effect on overall speech clarity. Preschool /s/ errors are expected and common. By the time a child enters kindergarten at age five, /s/ production should be mostly consistent. A child heading into first grade with significant /s/ errors is a good candidate for evaluation, particularly because reading instruction in that year leans heavily on phonological awareness of precisely these sounds.
The /th/ sound: the patient one
The /th/ sound is among the last to develop and one of the least concerning to watch and wait on. Errors on /th/ in kindergartners and even early first graders are entirely within the developmental range. Because /th/ is also relatively infrequent in English compared to sounds like /s/ or /r/, persistent errors on this sound alone rarely cause significant intelligibility problems. When /th/ errors persist past age seven or eight alongside other sound errors, they typically get addressed as part of broader articulation work.
What a “speech sound disorder” actually means
When a child’s speech sound errors persist beyond typical developmental windows in ways that affect intelligibility or communication, clinicians use the term speech sound disorder (SSD). This is an umbrella category that includes two main subtypes.
An articulation disorder involves difficulty producing specific sounds accurately at the level of motor execution. A phonological disorder involves difficulty with the underlying rule system of sound patterns, where a child applies systematic patterns (like always replacing sounds made in the back of the mouth with sounds made at the front) across many sounds rather than struggling with one sound in isolation.
This distinction matters because it shapes treatment. Articulation therapy focuses on motor placement and production practice. Phonological intervention works at the level of sound patterns and often produces faster generalization across multiple sounds simultaneously. A thorough speech evaluation distinguishes between these patterns and informs which approach will be most effective.
“Children do not outgrow speech sound disorders the way they outgrow shoes. Some patterns resolve naturally; others become more entrenched with time. Knowing the difference is exactly what a speech evaluation is designed to determine.”
What a speech evaluation at FOCUS looks like
A speech sound evaluation with a FOCUS Fort Myers speech therapist begins with a conversation about a child’s communication history, the specific sounds that prompted the referral, and how speech errors affect the child day to day. This context shapes how the evaluator approaches the assessment.
The evaluation itself is play-based and low-pressure. A speech-language pathologist elicits speech samples through conversation, picture naming, and structured activities designed to capture how the child produces sounds across different word positions (beginning, middle, and end of words) and in different contexts (single words, phrases, spontaneous conversation). For younger children especially, the session looks and feels like a game rather than a test.
The SLP also assesses oral motor structure and function, listening to how sounds are produced and observing the movement patterns of the lips, tongue, and jaw. This helps distinguish articulation errors from patterns that might involve structural considerations, such as a tongue tie, that could benefit from a different kind of intervention alongside or before speech therapy.
When early intervention makes the biggest difference
The research on speech sound disorders is consistent on one point: earlier intervention produces better outcomes. This is not because older children cannot make gains (they absolutely can), but because the developing brain in the preschool and early school years is at a particularly high point of neuroplasticity for language and motor learning. Patterns that take six months to shift in a five-year-old may take considerably longer to address in a nine-year-old who has had years of practice with a compensatory pattern.
There is also the question of literacy. Phonological awareness, the ability to hear and manipulate the sound structure of words, is the single strongest predictor of early reading success. Children with unresolved speech sound disorders frequently have underlying phonological awareness difficulties as well, and these can quietly shape a child’s reading trajectory before anyone connects the two. Addressing speech sounds in the preschool and kindergarten years is therefore not just a speech concern; it is a literacy investment.
- Speech therapy is most efficient when started before compensatory patterns become deeply habituated
- Preschool and early elementary years represent the highest window of motor and phonological learning
- Addressing /s/ and /r/ errors before third grade reduces the risk of spelling and reading difficulties downstream
- Children who feel understood communicate more, which accelerates language development across the board
- An evaluation with no clinical concerns is still useful information; it confirms that watching and waiting is the right call
Wondering about a specific sound?
A FOCUS speech-language pathologist can answer questions, help determine whether an evaluation makes sense, and walk families through what to expect from the process.
FOCUS Therapy offers Speech Therapy in Fort Myers, Florida. Call (239) 313.5049 or Contact Us online.
Additional Resources:
Singer, C., & Martin, E. (2023). “Treating a Young Child Who Stutters’ Lateral Lisp: A Case Study.” Perspectives of the ASHA Special Interest Groups. Read the study abstract here.
More Blog Entries:
Comments are closed.